

Design and participants
The sample comprised participants from the 2015 Pelotas Birth Cohort Study, a population-based cohort of all live births from mothers living in the urban area of Pelotas city, a median-sized city in southern Brazil. All women residents in the urban area of the city with confirmed pregnancy estimated delivery date in the year 2015 were invited to take part in the antenatal follow-up of the cohort. Eligible pregnant women were recruited from antenatal care health services, and face-to-face interviews were conducted using structured questionnaires. Information on depression during gestation was assessed mid-pregnancy (16–22 weeks).
From January 1 to December 31, 2015, maternity hospitals were visited daily, and all births were identified (over 99% of births in the city). In all, 4,333 live births were detected. Mothers of 4275 newborns (response rate 98.7%) agreed to enroll in the study and composed the final sample. Within 48 h after delivery, they replied to a face-to-face interview. At the age of three months, the children were visited at home by interviewers, and their mothers answered another questionnaire. A total of 4,110 3-month follow-up interviews were conducted (response rate 97.2%), of which 4,087 (95.6%) were carried out with the biological mothers. Figure 1 shows the 2015 Pelotas Birth Cohort recruitment and follow-up schedule. For the present study, we excluded from the analyses participants with conditions that could preclude breastfeeding or make it difficult, including women whose newborn was admitted to the intensive care unit, those who had twins, those who had a preterm delivery (< 37 weeks) and women diagnosed as being positive for human immunodeficiency virus (HIV). The final sample comprises data from 3,598 biological mothers. All information was collected through structured questionnaires applied face-to-face by interviewers who had completed undergraduate training. The interviewers participated in theoretical and practical training with, on average, two weeks of duration. Details about the methodology were previously published [25].

2015 Pelotas Birth Cohort recruitment and follow-up schedule adapted from Hallal et al. [17]
Measurements
Breastfeeding – outcome
This study explored breastfeeding in two different ways: (i) breastfeeding duration in months and (ii) attempt to breastfeed in the maternity unit. The first one was collected during the 12-month follow-up by asking “Until what age was the child breastfed?”. The range of responses varied from zero to 12 months. Due to the small number of children breastfed after eight months, we joined those breastfed for nine or more months into a unique category. Attempts to breastfeed while in the maternity ward were collected through the question “Have you already put the baby to the breast?” (response options “yes” or “no”).
Obstetric violence – exposure
Self-reported experience of obstetric violence was assessed during household interviews with the biological mothers three months after delivery. Due to the lack of consensus in the literature concerning its definition and the absence of validated instruments, we opted to operationalize obstetric violence as a latent variable composed of four items as described below.
Information on verbal abuse, physical abuse, negligence/denial of care, and undesired/non-consented procedures during hospitalization for childbirth were measured using the following questions: Verbal abuse: “Has any professional been rude to you, cursed you or yelled at you, humiliated you or threatened not to assist you?”; Physical abuse: “Has any professional ever pushed, hurt, beat, or held yourself strongly or conducted any examinations rudely or disrespectfully?”; Negligence/denial of care: “Has any professional refused to give you anything that you asked for, such as water or painkillers?”; Undesired/Non-consented procedures: “Has any professional ever conducted any procedure against your will, without explaining the need to conduct it, such as episiotomy or medication to induce labour?” To ensure that women would respond about events that occurred during the hospitalization for her most recent childbirth – subject matter of this study, the following introduction was included at the beginning of the obstetric violence questions block: “Now, let’s talk about the care you received during your hospitalization for the birth of your baby. To answer the next questions, consider what happened from the moment you arrived at the maternity ward until the moment you were discharged”.
Postpartum depression – mediator
Symptoms of postpartum depression were evaluated during face-to-face interviews conducted using the Edinburgh Postnatal Depression Scale (EPDS) three months after delivery. This scale comprises ten items, each scored on a 4-point Likert scale (ranging from 0 to 3), addressing common depressive symptoms experienced during the preceding week. A composite score is obtained by summing all item scores, resulting in a range from 0 (indicative of the absence of depressive symptoms) to 30 (denoting the highest score) [18]. A cut-off point of ≥ 13 points on the scale was employed to indicate the presence of at least moderate postpartum depression. Considering clinical interviews as the gold standard, this cut-off point has demonstrated a sensitivity of 59.6% (95% CI: 49.5–69.1) and specificity of 88.3% (95% CI: 83.9–91.9) for diagnosing depression [26].
The Cronbach alpha in this study was 0.796.
Potential confounders
According to the theoretical-operational model presented in Fig. 2, at the first level, we included as potential confounders woman’s age in years; marital status (living with a partner or not); woman’s educational level; socioeconomic position, and self-reported ethnicity. The women’s educational level was collected in completed years and categorized into 0 to 4, 5 to 8, 9 to 11 and 12 years or more. Socioeconomic position was evaluated according to the Brazilian Economic Classification Criteria (ABEP) on 01/01/2015 (available at and categorized into four economic groups: A (richest), B, C, and D/E (poorest). Self-reported ethnicity information was collected following the definition of the Brazilian Institute of Geography and Statistics (categorized as black, light-skinned black, white, Asian, and Indigenous) and categorized as white or non-white due to the small number of Indigenous and Asians in the sample. At the second level, we included antenatal depression measured by applying the EPDS between the 16th and 24th weeks of pregnancy. Positive screening for antenatal depression was defined as EPDS ≥ 10, which is the recommended cut-off for screening in the Brazilian population [26]. Last, the third level encompassed the delivery source payment (public or private) and parity, stratified in primiparous or multiparous women.
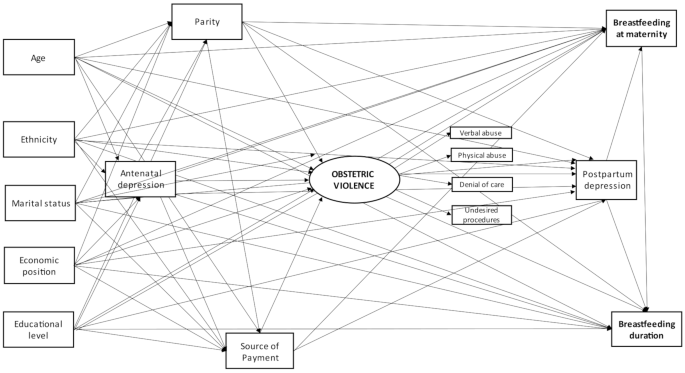
Theoretical-operational model concerning the relationship between obstetric violence and breastfeeding. This model was similar for women who underwent a vaginal and a c-section delivery
Statistical analyses
According to the literature, women who have a vaginal delivery present a higher probability of breastfeeding their newborn compared to those who have a c-Sect [21]. Therefore, we stratified all analyses by type of delivery.
First, we performed a descriptive analysis of socioeconomic and demographic characteristics. Hereafter, we described the prevalence of antenatal and postpartum depression and the prevalence of each item that composes the variable obstetric violence.
To evaluate the mediating effect of postpartum depression on the relationship between obstetric violence and breastfeeding, we performed structural equation models using Mplus 8.0. Obstetric violence was a continuous latent variable. We deemed a factor loading greater than 0.5 along with a p-value less than 0.05 indicative of a good correlation between the observed variable and the construct of interest [27]. This analysis employed weighted least squares mean, and variance adjusted (WLSMV) estimation, adopting theta parameterization. Considering the loss of information in some variables, we applied the full information method, encompassing the imputation of missing values.
We calculated modification indices using the MODINDICES command to obtain suggestions for changes to our initial hypotheses. Whenever proposed modifications (with modification rates greater than 10) were considered theoretically plausible, a new model was developed. In all analyses, we considered a path significant when the p-value was less than or equal to 0.05 [27].
We evaluated model fit employing the root mean square error of approximation (RMSEA), comparative fit index (CFI), and Tucker–Lewis index (TLI). The RMSEA compensates for model complexity by considering the adjustment given the number of parameters involved (i.e., degrees of freedom); values less than 0.06 indicate a good fit. RMSEA confidence limits greater than 90% and below 0.08 indicated a good fit. We inferred adequate model fit from CFI and TLI above 0.95 [28, 29]. Both the CFI and RMSEA are sensitive to the lack of model specification and are affected only slightly by sample size.
Ethics
This study was approved by the Research Ethics Committee of the School of Physical Education of the Federal University of Pelotas (CAAE 26746414.5.0000.5313) on February 5, 2014. All women provided written informed consent.
link




